

A pediatric contact lens fitting is a medical process, not a store purchase. If I’m helping a child start contacts, I need to look at readiness, eye measurements, lens type, safe handling, cleaning rules, and follow-up visits before daily wear begins.
Here’s the short version:
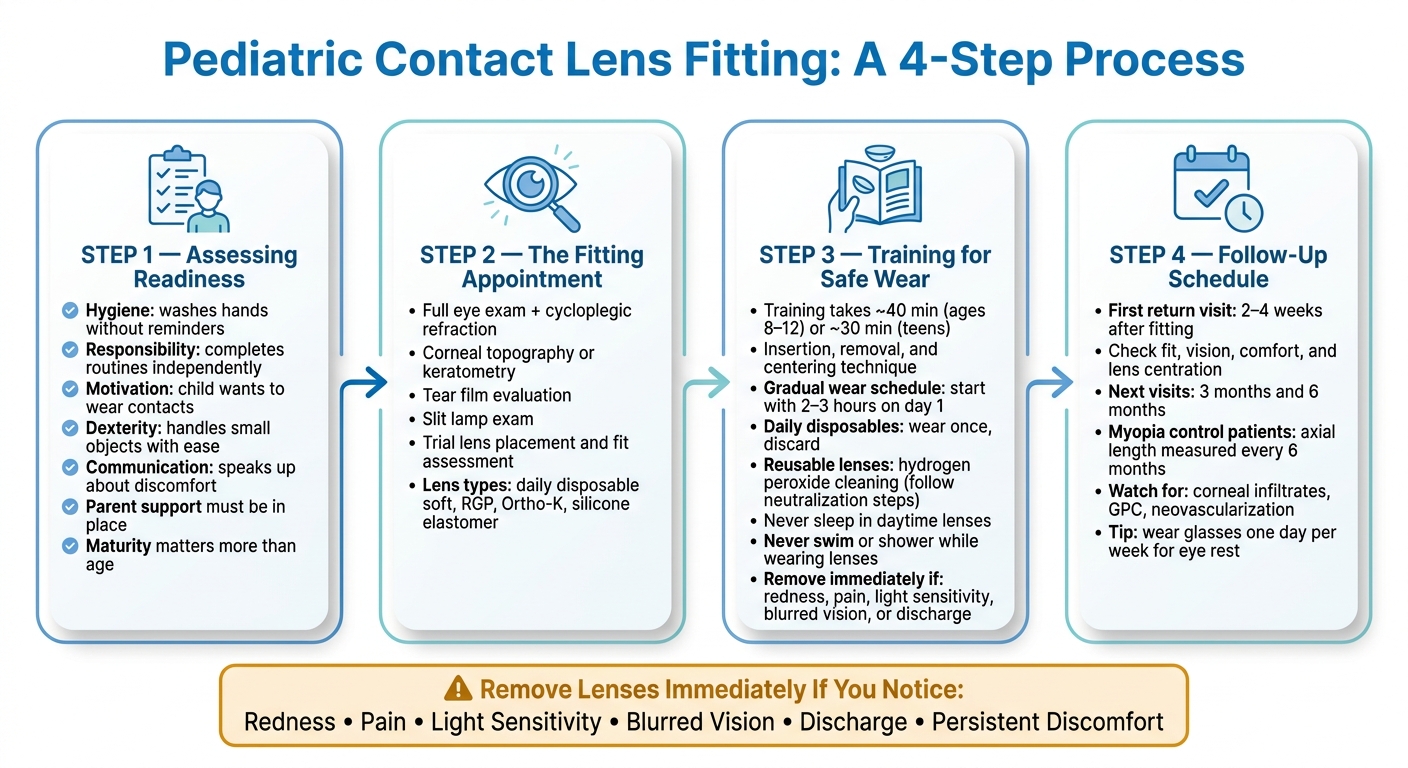
- I check if the child is ready based on hygiene, routine, motivation, eye health, and parent support
- I measure the eyes with an exam, refraction, and corneal checks to pick the right lens
- I teach insertion, removal, and care, which often takes about 30 to 40 minutes
- I set firm safety rules: no sleeping in daytime lenses and no swimming or showering in lenses
- I schedule a return visit in 2 to 4 weeks, then often again at 3 months and 6 months
- If there is redness, pain, light sensitivity, blurred vision, or discharge, the lens should come out right away and the eye doctor should be contacted
A child does not need to meet one set age. In many cases, maturity matters more than age. And if the first lens or first training session does not go well, that does not always mean contacts are off the table. Sometimes the fit, lens type, or timing just needs to change.
What matters most is simple: safe wear, clean hands, daily routine, and close parent involvement at home.
Pediatric Contact Lens Fitting: 4-Step Process Guide
Contact Lens Training and Fitting Video for a Child
sbb-itb-5ef6ec9
Step 1: Deciding If a Child Is a Good Candidate
The first call is pretty simple: can the child handle contact lenses in a safe, steady way?
Doctors don’t base that on age by itself. They look at maturity, hygiene, motivation, eye health, and how much parent support is in place.
Readiness Factors Doctors Evaluate
The biggest factor is motivation. The child needs to want contact lenses and be willing to take care of them. For non-medical wear, the child should be able to handle their lenses on their own.
Doctors also look at day-to-day habits. Does the child keep clean? Can they stick to routines without being chased down? Are they okay touching their own eyes? Eye issues such as dry eye, blocked oil glands, or severe allergies should be treated before lenses are fitted.
For medical cases, age may matter less. If a child has infant aphakia after cataract surgery or major anisometropia, contact lenses may be needed no matter where they are developmentally.
Signs of Readiness Parents Can Watch for at Home
Parents don’t have to wait for an appointment to get a rough sense of readiness. A few everyday habits can tell you a lot.
| Readiness Factor | What to Look for at Home |
|---|---|
| Hygiene | Washes hands often and keeps fingernails trimmed without reminders |
| Responsibility | Finishes homework or chores on a steady basis without help |
| Motivation | Keeps bringing up contact lenses and is willing to practice |
| Dexterity | Handles small objects and ties or fastens shoes alone |
| Communication | Speaks up about discomfort or problems instead of brushing them off |
Before the fitting, parents can have the child practice with eye drops and gently touching the area around the eye with clean fingers. That gives you a sense of how comfortable they are with eye contact and can make the visit feel less intimidating.
If a child has a hard time during the first training session, that doesn’t mean the answer is no forever. Doctors often check again in 4 to 6 months. The key point is simple: the child needs to be ready for the daily lens routine. Parents should back them up, not do the job for them.
If the child is ready, the next visit moves to measurements, trial lenses, and fit.
Step 2: What Happens During the Contact Lens Fitting
At the fitting visit, the doctor confirms the prescription, measures the eye, and picks a trial lens.
Eye Exam and Corneal Measurements
The visit begins with a full eye exam. First, the doctor checks visual acuity. Then they use cycloplegic refraction to find the true prescription by relaxing the eye’s focusing muscles.
After that, the doctor measures the surface of the eye in detail. Keratometry or corneal topography maps the curve of the cornea, which helps the doctor choose the right base curve for the lens. Horizontal iris diameter helps set the overall lens diameter. A tear film check looks for dryness that could make lenses less comfortable or harder to wear. A slit lamp exam checks the cornea, eyelids, and conjunctiva for swelling or allergies that could get in the way of lens wear. For children being fitted for myopia management, axial length measurement is often added to track how fast the eye is growing over time.
Choosing the Right Lens Type
The lens choice comes straight from those measurements and the child’s diagnosis. For many kids with nearsightedness, farsightedness, or astigmatism, daily disposable soft lenses are often the first pick. They’re easier to handle and remove the need for cleaning solutions.
If myopia control is the goal, the discussion may turn to peripheral defocus soft lenses or orthokeratology (Ortho-K) lenses worn overnight to reshape the cornea. For children with irregular corneas or high astigmatism, rigid gas permeable (GP) lenses often give sharper vision. Infants with aphakia after cataract surgery may need silicone elastomer lenses because they allow a very high level of oxygen through the lens.
Trial Lenses and Fit Assessment
Once the doctor chooses a lens type and size, they place trial lenses on the child’s eyes. After a short settling period, they check the fit under the slit lamp. The lens should sit in the right spot and move a little with each blink. If it barely moves, it may be too tight. If it moves too much, it may be too loose.
Then the doctor fine-tunes the prescription through the trial lens. They use extra lenses to confirm the best power for the child’s vision. This step matters even more with higher prescriptions, where small changes can make a big difference. Some families go home with a short trial supply before the final order.
The table below shows the main differences between the two lens categories most often used for pediatric patients:
| Feature | Soft Lenses | Rigid Gas Permeable Lenses |
|---|---|---|
| Comfort | Usually comfortable right away | Often less comfortable at first |
| Vision quality | Good for many common prescriptions | Often sharper for irregular corneas or higher astigmatism |
| Adaptation time | Short | Longer |
| Durability | More likely to tear | More durable |
| Typical pediatric use cases | General daily wear, sports, myopia management | Irregular corneas, keratoconus, aphakia, Ortho-K |
"Poor tolerability of one contact lens does not translate into the child not being ready for any contact lens. Rather, assess the fit, adjust the parameters, or consider another brand." – Noreen Shaikh, OD, FAAO
Once the fit is confirmed, the visit moves to insertion, removal, and daily care training.
Step 3: Teaching Safe Wear, Insertion, and Daily Care
Once the fit is confirmed, the visit moves into hands-on training.
Insertion and Removal Training for Children and Parents
When the lens fits well, the next job is teaching the child how to use it safely at home. A good fit matters, but it only helps if the child can handle the lens safely every single day.
Training usually takes about 40 minutes for children ages 8 to 12 and about 30 minutes for teenagers. During the school day, children need to be able to handle their lenses on their own. Before touching a lens, they should wash their hands well and keep their fingernails short so they don’t scratch the eye or tear the lens.
The doctor or technician shows the child how to hold the eyelids open, place the lens on the eye, and make sure it sits in the center. For removal, kids can use the method that works best for them:
- Pinch the lens out
- Slide it to the inner corner of the eye
- Use the eyelids to blink it out
At home, it helps to use the same setup each time: a table, a mirror, and all supplies in one spot. That small bit of routine can make the whole process feel less stressful.
Some children need a second training session, and that’s normal. Families are also sent home with written instruction sheets and signed care agreements so the routine stays clear.
Once the child can insert and remove the lens, the doctor sets the daily wear and cleaning routine.
Wear Schedule, Cleaning, and Water Safety
The child wears the lens. The parent makes sure the routine stays on track.
Some children do better with a gradual wear schedule, starting with just 2 to 3 hours on day one. Keep practice short on weekdays, then use weekends for longer wear sessions.
For daily disposable lenses, the rule is simple: wear them once, then throw them away. For reusable lenses like biweekly or monthly lenses, hydrogen peroxide-based cleaners can work well as a one-step disinfection option. But families have to follow the neutralization steps exactly. If they don’t, the cleaner can cause chemical burns.
Two rules apply to every child, no matter which lens type they wear.
- Daytime lenses must come out every night unless the doctor has specifically prescribed overnight wear. Sleeping in daytime lenses can lead to corneal injury and infection.
- Children should never swim or shower while wearing lenses. If a lens touches any water, it should come out right away to lower the risk of infection.
Symptoms That Mean Lenses Should Come Out Right Away
Families also need a plain, clear stop rule for symptoms that show up during wear.
They are taught to watch for redness, light sensitivity, vision changes, or pain. Discharge, heavy tearing, or discomfort that doesn’t go away are also signs to remove the lens at once.
If any of these symptoms show up, take the lens out and contact the eye care provider.
The next visit checks whether the routine is working and whether anything needs to change.
Step 4: Follow-Up Visits, Troubleshooting, and Long-Term Success
Follow-up visits help confirm that the lenses fit well, feel okay, and still give clear vision after a child starts wearing them at home. That early check matters. It can spot fit, comfort, or handling issues before they turn into bigger problems.
When Follow-Up Visits Usually Happen
The first return visit is usually set for 2 to 4 weeks after the initial fitting so the doctor can check fit, vision, and comfort. At that visit, the doctor looks at how the lens sits on the eye, makes sure it centers well, and checks that it moves a little with each blink. They also confirm that the prescription is still right.
If all looks fine, the next visits are often scheduled at the 3-month and 6-month marks to watch for complications. During these visits, the doctor uses a slit lamp to look for early signs of trouble, including corneal infiltrates, neovascularization, allergic reactions such as giant papillary conjunctivitis, and mechanical trauma.
Kids using lenses for myopia control, such as MiSight or orthokeratology lenses, need closer checks. Axial length measurements are often taken every 6 months to track eye growth and see how the treatment is going.
Common Contact Lens Problems and What to Do
Between visits, families should treat changes in comfort, redness, or vision like a stop sign. If something feels off, take it seriously. The table below shows common at-home warning signs and what to do next.
| Problem | Immediate next step | When to call the clinic |
|---|---|---|
| Blurry vision | Remove the lens and inspect it for deposits or damage; clean or replace it if needed | Call if the blur does not clear after the lens is removed or replaced |
| Discomfort or irritation | Remove the lens right away and do not reinsert it until the cause is clear | Call the same day if the discomfort does not improve quickly |
| Redness | Remove the lens immediately and stop wearing lenses | Call promptly, especially if redness is paired with pain, light sensitivity, or discharge |
| Itching with stringy mucus or discharge | Remove lenses and have the eyes evaluated for possible giant papillary conjunctivitis (GPC) | Call for a follow-up visit and possible break from lens wear |
| Dryness | Use only doctor-approved, unpreserved lubricating drops if they have been recommended and reduce wear time | Call if dryness is frequent or worsens |
What Families Should Remember
Pediatric contact lens fittings depend on readiness, proper fit, hands-on training, and steady follow-up.
"Young patients often require parental involvement in their contact lens care… parents’ engagement and understanding of the risks and proper techniques for contact lens care contribute to the lower rate of contact lens complications among children." – Noreen Shaikh, OD, FAAO
A simple habit can help with long-term lens wear: have the child wear glasses one day a week. That keeps the backup pair up to date and gives the eyes a regular break from lenses.
FAQs
How do I know if my child is ready for contacts?
Readiness for contact lenses has less to do with age and more to do with your child’s motivation and maturity. A child who wants to wear contacts – and understands that they come with daily care – is usually in a much better spot than one who’s just asking on a whim.
A good candidate can handle hygiene and lens care without cutting corners. That means solid hand-washing and nail-trimming habits, taking care of their glasses, and having the patience and fine motor control to insert, remove, and clean lenses.
What type of contact lenses are best for kids?
The best contact lens for a child depends on their vision needs and overall eye health. For common refractive errors like myopia, hyperopia, and regular astigmatism, soft lenses are usually the most common pick.
When it makes sense, daily disposable lenses are often recommended because they make hygiene easier and can lower the risk of infection. For medical or more complex needs, specialists may use silicone elastomer, rigid gas permeable, scleral, orthokeratology, or custom soft lenses.
What should I do if my child has pain or redness with contacts?
Have your child stop wearing the lenses right away.
Pain or redness can point to anything from mild irritation or allergies to a more serious infection. Contact your eye care provider at Eye Center of Northern Colorado as soon as you can for an evaluation, and do not start lens wear again until you’ve spoken with your doctor.


